
TN-401
Our clinical-stage gene therapy for PKP2-associated ARVC
Mutations in plakophilin-2 are the most common genetic cause of ARVC, resulting insufficient levels of critical desmosomal proteins needed to maintain the structural integrity and cell-to-cell signaling of heart muscle cells. TN-401 gene replacement therapy is designed address the underlying cause of disease by delivering a working PKP2 gene to the heart.
ARVC and Genetics
How TN-401 Works
RIDGETM-1 Phase 1b Clinical Trial
Tenaya’s Non-interventional Study for PKP2-Associated ARVC
Frequently asked questions
Understanding AAV-based Gene Therapy
How many patients have been treated with AAV9-based gene therapies around the world?
What is the difference between gene therapy (replacement) and gene editing?
How does AAV gene therapy differ from COVID vaccines?
How does gene therapy produce the missing protein?
Gene Therapy Safety
What immunosuppression regimens are being used for AAV gene therapies?
What happens to the AAV9 viral capsid after infusion?
Is AAV9 transmissible to household contacts/family members?
What are the most common side effects associated with AAV-based gene therapy and how often do they occur?
What is the risk of myocarditis with AAV gene therapy?
What is the risk of mutagenesis with AAV gene therapy?
TN-401 General Aspects
Basic explanation of gene therapy construct formation/how is this manufactured?
Why did Tenaya Therapeutics select AAV9 to treat PKP2-associated ARVC?
Why don’t you administer TN-401 through an intra-coronary route vs. intravenous (IV)?
Does TN-401 alter the patient’s genome (integration)?
Are patients able to be re-dosed with TN-401?
Will patients be able to stop their medications and avoid cardiac interventions after TN-401?
Does the patient continue to make dysfunctional protein alongside WT protein after TN-401 has been administered? Can dysfunctional protein compete with TN-401-derived WT protein within the sarcomere?
Does it matter which PKP2 mutation an individual has in order for TN-401 to benefit?
How long does it take for the gene therapy to demonstrate benefit?
How long will the effect of TN-401 last?
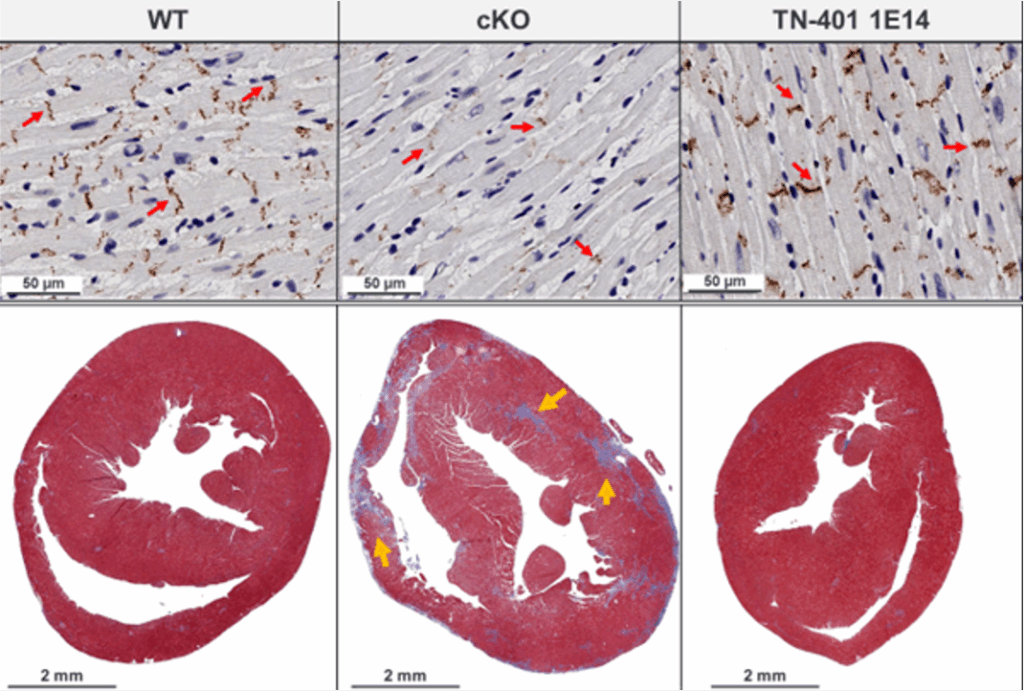
The KO mouse model is homozygous and doesn’t accurately represent the heterozygous humans you will be studying in the RIDGETM-1 clinical trial. Will study participants see similar degrees of efficacy?
Will TN-401 work if the heart has too much fibrosis?
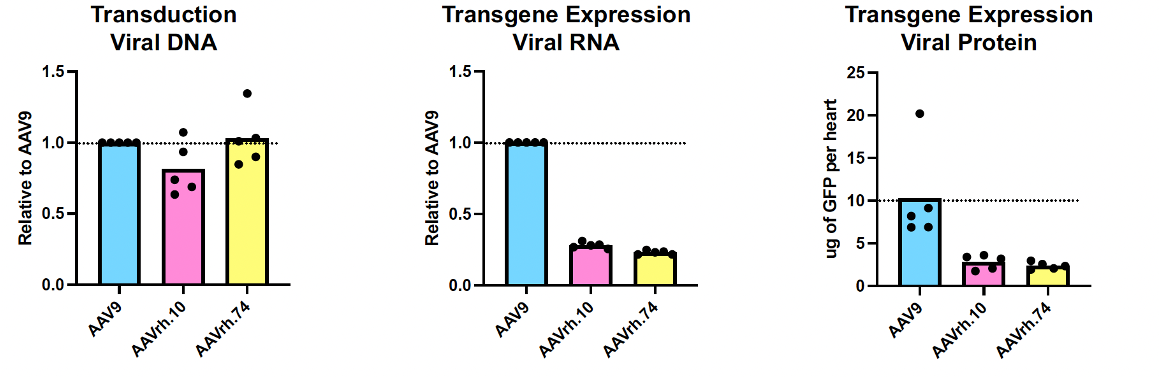
How do you measure the transgene expression to determine if PKP2 expression is restored?
Is there a way to remove the transgene after it has been administered?
TN-401 Safety
How often has TMA occurred with gene therapy?
What is the risk of overexpressing PKP2 protein following TN-401 therapy?
How much PKP2 protein levels could be enough for normal heart function?
Do we anticipate seeing a drop in ejection fraction in human subjects following the infusion of TN-401?
Is transgene expressed in other off-target tissues like the liver?
Are patients at increased risk if they have had myocarditis following the COVID-19 vaccine?
How long does the patient need to take immunosuppression?
Are the patients eligible for heart transplant after the AAV gene therapy?